RALPH Lataster of the University of Sydney recently published a paper in the International Journal of Risk and Safety in Medicine on excess deaths in Australia.
He concluded that: ‘Combined with increasing evidence that the efficacy/effectiveness and safety of Covid-19 vaccines have been greatly exaggerated, including acknowledgements from the Australian and American governments that several deaths have been caused by the vaccines, these findings make it a near-certainty that Covid-19 vaccines have been – and continue to be – contributing to excess mortality.’
His analysis focused on four regions: Queensland, Western Australia, South Australia and the Northern Territory. He says they didn’t have a ‘covid problem’ and didn’t do much by way of lockdowns, making them as close to a control group for the rest of Australia as possible (bearing in mind that Australia was infamous for some of the harshest lockdowns during the so-called pandemic).
In his substack Okay the News Lataster says: ‘No doubt partly because of the country’s relative isolation and natural oceanic borders, in the regions of Queensland, Western Australia, South Australia and the Northern Territory, deaths from Covid-19 only became a (relatively) big deal from 2022 onwards.’
He looks at the mortality patterns in the period across these territories and concludes: ‘The typical explanations involving Covid-19 and lockdowns do not adequately explain the extent of excess mortality in several regions of Australia during 2021. Given that these regions vaccinated just as rapidly and thoroughly during 2021 as the rest of the country, as well as the increasing evidence published in the literature that the vaccines do cause serious adverse effects and even death, it is incontestable that mass vaccination with Covid-19 vaccines is at least partially responsible for excess mortality. More research is urgently required, perhaps focusing on the general health and mortality of the vaccinated (including Covid-19 mortality), as compared with the unvaccinated.’
The mortality difference between 2020 and 2022 in Australia is startling:

In 2020 we have negative excess deaths (during a global pandemic) but 11.7 per cent excess deaths in 2022, post vaccine roll out. And note that excess deaths in 2022 were significantly higher than covid deaths.
The covid statistics mortality for the Northern Territory is representative of all of low lockdown, low covid Australian states. It had zero covid deaths in 2020, yet had an excess of almost 20 per cent in 2022.

The vast majority of eligible Northern Territorians aged 16 and up received at least one covid vaccine dose by the end of 2021, 89.3 per cent. This high rate of vaccine uptake was more or less the same throughout Australia.
Lataster points out that: ‘Considering the period 2020-2021, as excess mortality across the four regions increased, Covid-19 mortality decreased, strongly indicating that Covid-19 is not to blame, making it relatively likely that Covid-19 interventions are behind the rise in excess mortality in 2021.’
Astute readers will recall that we conducted a mortality analysis back in December 2022, which included Australia. In our study we compared covid cases worldwide with excess mortality showing they diverged:

At that time we offered the (preliminary) conclusion that the vaccines were to blame, so we are very pleased that Lataster’s analysis has confirmed our conclusions, and are also pleased that his work has made it into print.
This is all very good news and Lataster deserves much credit for his persistence and hard work in getting this into print. However the rot goes way deeper.
Lataster quite rightly makes the point that covid deaths were hyped, saying: ‘Blaming Covid-19 is risky because we would have to have been undercounting Covid-19 deaths, by a lot, when the evidence indicates the opposite, that Covid-19 deaths have been hyped up.’
Calling this an understatement is putting it mildly. Our view is straightforward: there was no unique ‘covid disease’, no genuinely novel virus and no pandemic in the sense we were told. What unfolded was driven by flawed science, questionable statistics and testing practices that shaped the narrative rather than clarified it.
If a pandemic was truly sweeping the globe, why did remote and isolated regions of Australia see almost no covid at all? And why did some densely populated parts of Europe — Northern Ireland being a prime example — also experience minimal impact? These aren’t fringe locations, they’re major populations that simply didn’t match the story.
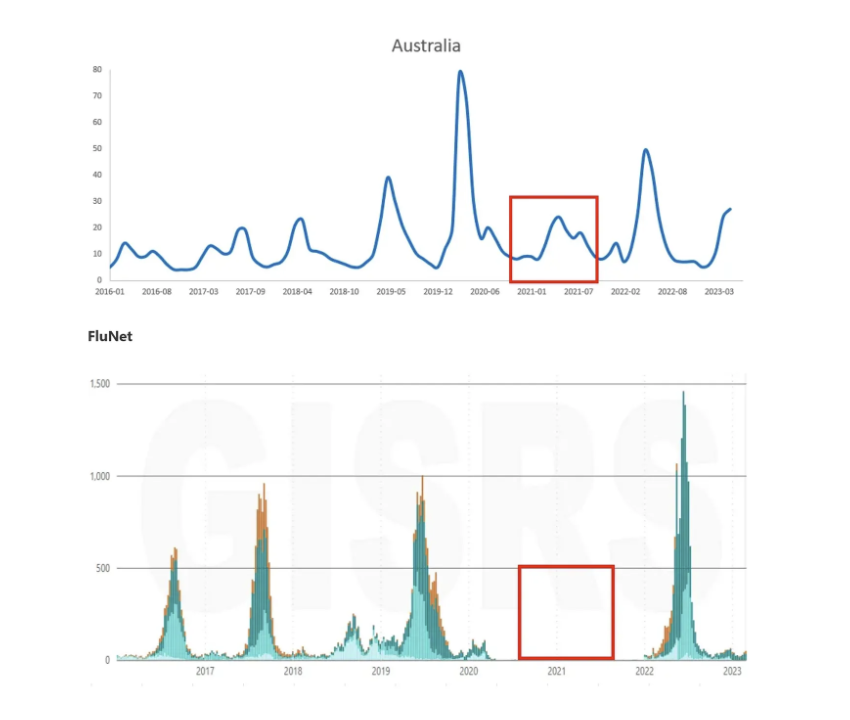
The assumption behind the ‘remote Australia’ explanation is that isolation protected those areas in 2020. But if isolation was the magic shield, it should have blocked influenza as well. Did it?
According to FluNet, influenza supposedly vanished from Australia in mid‑2020 and stayed away throughout 2021. Yet Australians were still searching for flu information on Google the whole time. Why would people be looking up a virus that had supposedly disappeared from the country?
The inconsistencies speak for themselves.
This was not an uncommon pattern, with flu supposedly disappearing worldwide, as we report in this article, and in others. What was actually spreading was the suppression and manipulation of flu tests and statistics. There is evidence of widespread manipulation of causes of respiratory death, as reported here.
In 2020, influenza and pneumonia deaths in Australia were about 60 per cent of the 2019 numbers. So yes, 2020 looked like a ‘good’ year for respiratory infections compared with 2019, which was unusually bad. But people were still dying from illnesses grouped under the influenza‑and‑pneumonia category even during the covid period, and not all of those deaths were labelled as covid.
What stands out is this: even though Australia reported extremely low levels of influenza and SARS‑CoV‑2 circulating in 2020, the overall flu‑and‑pneumonia death rate barely moved. At the same time, the proportion of pneumonia deaths attributed to an ‘unknown’ cause jumped from an already high 70 per cent in 2019 to 94 per cent in 2020.
That naturally raises questions. Why would classifying pneumonia cases suddenly become harder in 2020 than in 2019? And if flu and SARS‑CoV‑2 supposedly weren’t circulating, why were pneumonia numbers so similar across both years?
This is where the story gets contradictory. We’re told that lockdowns and border controls kept Australia ‘safe’ from SARS‑CoV‑2 in 2020, in effect sealing the country off. Yet somehow flu and pneumonia carried on almost unchanged. So did the restrictions work for one virus but not the other? That doesn’t add up.
Australia’s pneumonia mortality rates in 2020 also lined up closely with those in the US and UK. That consistency suggests there wasn’t a dramatic shift in overall respiratory mortality, and it challenges the idea that 2020 represented an acute and unique respiratory crisis in any of those countries.
And it’s worth remembering that hospital testing practices changed during the pandemic. In several countries — including the US, UK, Germany and Australia — routine flu testing was scaled back or deprioritised. That inevitably affected how respiratory illnesses were classified.
Things get worse. The way Australia calculated excess deaths was manipulated as reported here. In this article we said: ‘We see the same in Australia where they estimate 2022 excess deaths using 2017-2019 and 2021 but do not include 2020. But in Australia 2020 was actually a normal year, despite the fact that the Australian Bureau of Statistics stated “2020 has been excluded as it did not resemble a typical mortality year. So, by including a year that is higher than expected and excluding a normal year, the excess is manipulated to look smaller”.’
The idea that excess death baselines were ‘expected’ is an understatement. Those baselines were adjusted in ways that conveniently made the situation look better than it was.
When the actual excess, culled from the Australian Bureau of Statistics data, is compared with that from previous decades the excess mortality signal from 2022 is stunning:

For a long stretch, anyone wanting to publish on covid had to sign up to the full package: the vaccines were safe and effective, and covid itself had to be treated as an unquestionable reality, though variations around the appropriateness of the ‘response’ and the level of the ‘threat’ were permissible, provided the existence of some sort of threat was not totally denied. That was the entry ticket.
Now the landscape has shifted. It’s become acceptable to criticise the covid vaccines — but only if you stop short of questioning the underlying covid narrative itself. While being labelled an ‘anti‑vaxxer’ might be becoming tolerable, being seen as a ‘covid denier’ is still off‑limits.
Two later sections of Lataster’s paper show exactly how this pressure works. He still aligns himself with two key pillars of the mainstream story: the central role of the spike protein, and the idea that different ‘variants’ had distinct effects on mortality. Whether he does this willingly or because it’s the only way to get published, the result is the same — the narrative boundaries remain firmly in place.
Lataster notes that the medical authorities might be tempted to argue that ‘perhaps the easiest and most plausible explanation is that virtually all the excess deaths are covid deaths, that the latter has somehow been underestimated’.
What lets this whole line of reasoning survive is the idea that the spike protein is some kind of hidden, insidious threat — dangerous no matter how it enters the body, whether through a virus or a vaccine. Under that logic, virtually everyone was exposed to the SARS‑CoV‑2 spike protein, even if they never felt a thing. The claim then follows that this silent exposure was the real cause of later illness, with the supposed excess mortality only becoming visible over time.
It’s a convenient narrative — having your cake and eating it.
But is the spike protein really the culprit? We’ve argued before that there’s nothing uniquely alarming about the spike protein, or any other component of SARS‑CoV‑2 for that matter. In reality, there’s nothing particularly novel or risk‑enhancing about SARS‑CoV‑2 at all, and it can be coherently argued that it is not a ‘thing’ at all but simply an artificial sequence.
On the question of variants, Lataster makes some interesting points when comparing Bulgaria and Australia, a contrast we also highlighted in our 2022 mortality analysis.
He says: ‘While vaccine deaths occurred in Bulgaria for several years post-vaccine rollout, more lives from Bulgaria’s relatively elderly population could have been saved by the vaccines initially. The situation differs in Australia, with its younger population, and having more of an exposure to the later variants . . .’
The problem is that the whole variants narrative is largely nonsense. They cannot be isolated from a co-evolving viral swarm. Leaning on it only reinforces the broader mythology: the idea of pandemics as inevitable, recurring threats and the supposed need for a permanent biosecurity framework to manage them.
And of course, this logic conveniently lets them off the hook. With this framing, they can always claim the vaccines ‘worked’, just not under the exact circumstances in which they were deployed. The problem, they’ll say, wasn’t the product itself but the timing. Get the vaccines to market faster, line them up with the supposedly deadly variants, and suddenly the narrative becomes that countless lives would have been saved.
It’s (another) tidy way to protect the story and shift responsibility away from the people who rolled out the products.
This article appeared in Where are the Numbers? on February 24, 2026, and is republished by kind permission.