

The Japanese have a saying: ada yori takai mono wa nai. Translated, which is the only way I know how to read Japanese, it means “there is nothing so expensive as something that is free.”
There ain’t no free lunch, which is the less elegant American version.
Our Anglo-American friends are very proud of their “free” health care systems, and American lefties firmly believe that the United States is backwards and tyrannical because we don’t have one of our own.
Far be it from me to vigorously defend America’s byzantine health care finance system, which is a Rube Goldberg abomination in which government agencies, politicians, and insurance companies conspire against ordinary Americans to make it outrageously expensive, but few Americans would tolerate what is standard practice in places like Canada or the UK when it comes to getting treatment for diseases.
In Canada, it is becoming common for doctors to recommend assisted suicide for treatable conditions. A healthy but elderly woman went to the hospital with back pain, and even before she was examined, she was offered suicide.
The government-run program is getting faster and making approval easier to get, writes Rupa Subramanya. MAID deaths since Canada made them legal could soon approach 110,000. https://t.co/EYHMlql0Hh
— The Free Press (@TheFP) March 5, 2026
Murdering patients is much cheaper than treating them, so people with PTSD, mental illness, or disabilities are offered death as a treatment.
The House of Lords killed a bill to bring MAiD to Great Britain, to the disappointment of many Labour Party members who now want to reform the upper house to make passing such laws easier. Still, waiting lists to see doctors and get treatment are excruciatingly long, with many people dying before being seen, and it is a political problem for Labour.
Their solution? Reduce the size of the waiting lists by stopping referrals to hospitals and specialists.
.@NHS, objectively the worst access & outcomes of all, yet considered a model by @BernieSanders & blind advocates of single-payer, continues to fail https://t.co/gzL0krpfuC
— The Independent with Scott Atlas (@ScottAtlas_IT) March 29, 2026
Instead of being on a waitlist, you are denied any care at all.
The NHS is to ration hospital referrals as Labour scrambles to meet its pledge to cut waiting lists.
GPs have been ordered to consult on at least one in four referrals rather than sending them to hospital in order to reduce “unnecessary” appointments.
The quotas, the latest method the NHS is using to keep waiting lists down, will come into force on Wednesday.
But MPs and medics have raised concerns that setting an arbitrary target will delay patients from getting access to the healthcare they need.
Dr Luke Evans, shadow health minister and a former GP, told The Telegraph: “My biggest concern is about this single point of access, with a target to bounce back one in four referrals – that is bad for clinicians and it is really bad for patients.
“It is hard not to see this as a way of Wes Streeting simply controlling access to hospitals and massaging waiting lists.
“We don’t even know if the planned 1 in 4 patients bounced back to the GP are recorded. Is Labour planning on effectively rationing secondary care – it seems like it.”
Shocked? I’m not.
For years in the first decade of the century, the VA was held up as a model for what a universal healthcare system should look like in the United States. It had low wait times, great outcomes, and low costs per patient.
I remember following the stories and wondering, “Do they have a point?” The answer was no. It was all a fraud. Waitlists were manipulated, as were the stats. People were dying, and because they died, the waitlist got shorter. Success!
This is how bureaucracies think, and how political hacks cover their own rear ends.
The NHS is just doing the same thing here. Whenever you measure something, you get a system oriented toward hitting the numbers. This can be good or bad. It depends on whether you are measuring the right thing.
In healthcare, you should measure customer satisfaction and health outcomes first, along with a measure that aims toward efficiency in the delivery of services. If you are measuring wait times, you will focus on wait times, and the easiest way to achieve your goal is to deny service entirely.
No waiting! Sure, people are in pain, or dying, or living in fear. Their health may suffer. But the bureaucrats hit their numbers.
Visit any website of a welfare agency, and they will often brag about how many clients they have, not how many people they have helped out of poverty. The metric is wrong, of course.
In the American healthcare system, outside Emergency Care at least, customer satisfaction tends to be pretty high and the services are quite good, at least in Minnesota. But there are all sorts of indications that I am not the customer—it’s the insurer, and to a great extent, the government. Health care systems compete for customers because they generate revenue, but what they really want are people to treat.
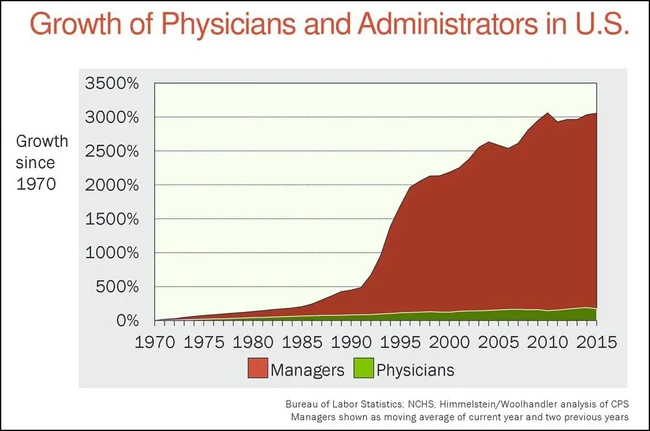
That’s why the growth in healthcare administrators has been astronomical, while the number of actual healthcare providers has barely increased compared to the population.
Administrators exist to please the customer, and that customer is the bureaucracy in insurance companies or the government. They employ doctors as an excuse to deal with their customers.
I could spend hours, days, or weeks going into how we got here in the United States, and I honestly don’t know how you get from here to a freer market system, but there are people who know much more than I do about both.
But it’s clear that all the hype about government-run healthcare is based on crap data. Canada may do a decent job, for all I know, providing basic healthcare and fixing broken bones, but any system that has to resort to killing people to hold down costs is fundamentally broken.
Liberals don’t see this because they are so blinded by ideology that they come up with crazy ideas like “Cuba does a great job!” Or, at best, they are tricked into looking at the wrong metrics or not understanding basic things like the differences between how the US measures things versus other countries. For instance, we take extraordinary measures to save babies in neonatal ICUs. Many countries count these babies as stillborn and exclude them from infant mortality statistics.
Again, not to get too deep in the weeds, I have little doubt that Britain will lower the stats for wait times. But only because they abandon many patients to lingering deaths, great pain, or the fear of wondering whether they have cancer.
That’s not an achievement.
Editor’s note: If we thought our job in pushing back against the Academia/media/Democrat censorship complex was over with the election, think again. This is going to be a long fight. If you want to join the conversation in the comments — and support independent platforms — why not join our VIP Membership program? Choose VIP to support Hot Air and access our premium content, VIP Gold to extend your access to all Townhall Media platforms and participate in this show, or VIP Platinum to get access to even more content and discounts on merchandise. Use the promo code FIGHT to join or to upgrade your existing membership level today, and get 60% off!









